Blog
What Is a Screening Panel? A Healthcare Guide

TL;DR:
- A screening panel is a grouped set of tests that detects multiple substances or conditions from one specimen efficiently.
- Understanding panel types, purposes, and regulatory context ensures proper clinical use and avoids misinterpretation.
Most healthcare professionals have ordered a drug screening panel without stopping to question what actually defines one. A screening panel is a grouped set of tests designed to detect multiple substances or conditions from a single specimen in a single workflow. That distinction matters more than it sounds. Understanding the screening panel definition, how panels are structured, and how results should be interpreted separates clinicians who use them well from those who rely on them blindly. This guide covers types of screening panels, how they work, regulatory context, and what you need to know to use them accurately in clinical or organizational practice.
Table of Contents
- Key Takeaways
- What is a screening panel in drug testing
- Types of screening panels
- Why screening panels are used
- How screening panels work from collection to results
- My take on screening panels after years in this space
- Drug test panels built for healthcare organizations
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Screening panel definition | A panel groups multiple tests into one workflow, increasing efficiency without requiring multiple specimens. |
| Types vary significantly | From 5-panel drug tests to 22-panel cups, panel selection must match clinical or compliance goals. |
| Purpose drives design | Panels exist to detect, not diagnose. Positive results always require confirmatory testing before action. |
| Regulatory context is critical | Panel recommendations from bodies like the USPSTF directly affect insurance coverage and patient costs. |
| Consent is non-negotiable | Patients must give informed consent before screening, even in high-volume clinical environments. |
What is a screening panel in drug testing
A screening panel is a single test containing multiple analyte targets, each with its own detection threshold, that produces results for all included substances from one specimen collection. In drug testing, this means a urine sample collected once can be analyzed for amphetamines, opioids, benzodiazepines, THC, cocaine metabolites, and more, all at the same time.
The contrast with single-substance testing is significant. A standalone THC test tells you one thing. A multi-panel drug test tells you whether the patient or employee has multiple substances present, which is far more relevant for clinical decisions, compliance programs, and treatment planning. Multi-panel tests improve testing efficiency and accuracy by detecting multiple substances simultaneously rather than requiring sequential testing.
Standard drug screening panels used in healthcare and workplace settings typically include:
- Amphetamines (AMP): Covers methamphetamine and prescription stimulants
- Cannabinoids (THC): Detects marijuana metabolites
- Cocaine (COC): Flags benzoylecgonine, the primary cocaine metabolite
- Opiates (OPI/OPI2000): Covers morphine, codeine, and heroin-related compounds
- Phencyclidine (PCP): Detects dissociative drug use
- Benzodiazepines (BZO): Commonly added for clinical populations on sedative medications
- Oxycodone (OXY): Not always captured by standard opiate screens; often requires a separate target
Pro Tip: When selecting a panel for a pain management clinic, always verify whether oxycodone is included as a discrete target. Standard opiate screens miss it at clinically meaningful thresholds.
Types of screening panels
Panel selection is not a default decision. The range of test panel types available reflects genuinely different clinical needs, regulatory requirements, and risk profiles.
Standard drug test panels
The most common configurations in healthcare and workplace settings are structured around panel count, which refers to the number of drug classes being screened.
| Panel | Typical drugs covered | Common use case |
|---|---|---|
| 5-panel | THC, cocaine, opiates, amphetamines, PCP | DOT-regulated workplace testing |
| 10-panel | Above plus barbiturates, BZO, methadone, propoxyphene, methaqualone | General employment screening |
| 12-panel | Above plus oxycodone and MDMA | Clinical and substance abuse programs |
| 15-panel | Expands to include buprenorphine, tramadol, fentanyl, ketamine | Pain management and addiction medicine |
| 22-panel | Adds designer drugs, Zaza (tianeptine), and adulterant checks | Forensic, high-risk clinical environments |
Each step up in panel count adds analyte targets that matter in specific contexts but may be unnecessary noise in others. A 22-panel screen run on every pre-employment candidate at a landscaping company is wasteful and raises legal exposure. The same panel at a medication-assisted treatment clinic is clinically defensible.
Expanded and customized panels
Beyond standard configurations, labs and point-of-care manufacturers offer customized panels. These are built for organizations with specific compliance needs or patient populations. A forensic toxicology lab serving courts, for instance, may run panels that include synthetic cannabinoids, novel opioids like nitazenes, or specific designer benzodiazepines not on any standard panel.
The expanded carrier screening market will reach $5.3 billion by 2030, with predesigned panels accounting for 62% of that value. That figure reflects a broader truth: standardized, prebuilt panels dominate adoption because they lower cost and speed up implementation.
Clinical and newborn screening panels
In clinical medicine, screening panels extend beyond drug testing to genetic and metabolic conditions. The U.S. Recommended Uniform Screening Panel currently lists 38 core and 26 secondary conditions for newborn screening. Core conditions meet strict criteria: they must be detectable by sensitive tests, have well-understood outcomes, and have effective treatments available. Secondary conditions are often identified incidentally during testing for core conditions and may lack effective treatment or clear clinical guidance.

Critically, only 2 of 56 state and territorial programs screen for all 38 core conditions, which means the panel a patient receives depends heavily on geography. For healthcare organizations operating across state lines, that inconsistency requires active management.
There is also a meaningful shift happening in genetic carrier screening. Panethnic screening panels are increasingly replacing ethnic-specific panels because ethnicity is difficult to determine reliably, and ancestry-based approaches create accuracy gaps that disadvantage patients. The move toward panethnic panels reflects a commitment to equitable screening access across all patient populations.
Why screening panels are used
Understanding the purpose of screening panels prevents organizations from treating them as a checkbox rather than a clinical tool.
- Early identification. Panels catch substance use, metabolic abnormalities, or genetic conditions before symptoms appear or before a single-substance test would be ordered.
- Treatment planning support. A positive result on a multi-substance panel gives clinicians a complete picture of what a patient is using, not just confirmation of one suspected drug.
- Workplace and regulatory compliance. Federal agencies mandate specific panel configurations for safety-sensitive positions. Using the wrong panel creates compliance liability.
- Insurance and coverage alignment. USPSTF panel recommendations directly shape what the Affordable Care Act covers as preventive care. When panel composition changes at the federal level, patient out-of-pocket costs shift accordingly.
- Population-level monitoring. In public health and clinical research, panels provide aggregate data on substance use trends, treatment adherence, and emerging drug threats.
The importance of screening panels in healthcare goes beyond individual test results. They shape national preventive care standards, influence clinical decision pathways, and carry direct financial consequences for patients based on which body recommended the panel and when.
Pro Tip: Before deploying a panel for your organization, cross-reference its substance list with your state’s current regulatory requirements and your patient population’s known risk profile. A panel that does not match both factors wastes money and may create legal exposure.
Knowing how to select test panels is as important as understanding what a panel detects. Poorly matched panels generate false reassurance or unnecessary follow-up testing, both of which cost organizations time and credibility.
How screening panels work from collection to results
The workflow for a drug screening panel follows a defined sequence. Understanding each step helps you catch errors before they reach the patient or compliance record.
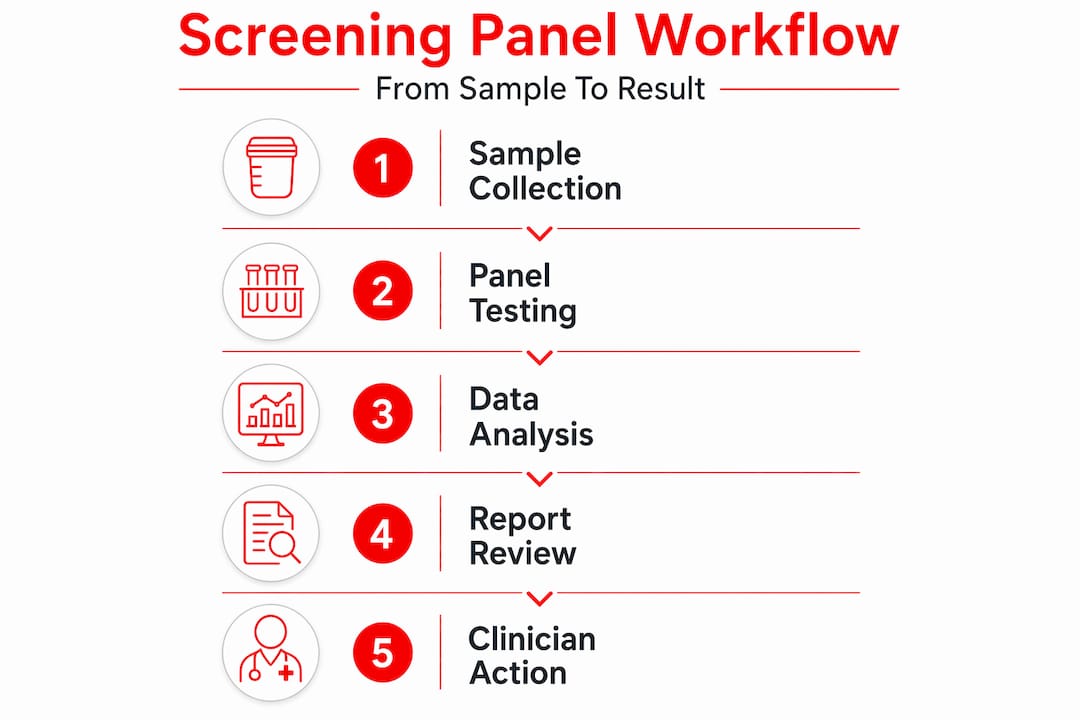
Specimen collection is where most errors originate. Urine is the standard matrix for most drug panels at the point of care. Oral fluid, blood, and hair each offer different detection windows and have different chain-of-custody requirements. For workplace and forensic applications, observed collection or temperature verification is required to establish specimen validity.
Testing technology at the point of care relies on immunoassay, a competitive binding method that produces a rapid qualitative result. Most drug test cups operate this way. Laboratory-based confirmatory testing uses gas chromatography-mass spectrometry (GC-MS) or liquid chromatography-tandem mass spectrometry (LC-MS/MS), both of which provide quantitative results and definitive substance identification.
Results from an initial screen are categorized as follows:
- Negative: The analyte was not detected above the cutoff threshold. This does not mean zero presence; it means the level was below the detection limit.
- Positive (presumptive): The analyte exceeded the cutoff concentration. Requires confirmatory testing before any adverse action.
- Invalid or adulterated: The specimen shows signs of tampering, dilution, or substitution. Panels with adulterant detection strips flag this at the point of collection.
Secondary findings, which are results that were not the primary target of the screen, require careful handling. Secondary conditions detected incidentally can affect follow-up care even when they were not the reason for testing.
On consent: screening tests are voluntary, and patients must give informed consent before any screening occurs, including drug testing in clinical contexts. High-volume environments create pressure to skip this step. That is a legal and ethical risk that organizations routinely underestimate.
My take on screening panels after years in this space
I’ve watched healthcare organizations tie themselves in knots over screening panels because they treat panel selection as an IT procurement decision rather than a clinical one. Someone picks the cheapest cup that clears compliance on paper, and then a pain management patient tests negative on a fentanyl screen because fentanyl was never on the panel they ordered. That is a real clinical failure, and it happens constantly.
What I’ve learned is that the most important question to ask is not “what does this panel test for?” but “what is this panel likely to miss given our patient population?” The gap between those two questions is where clinical judgment lives.
I’m also concerned about the standardization problem. The fact that implementation lag for new conditions on federal screening panels can stretch years means organizations are often working with outdated evidence even when they think they are current. Staying compliant is not the same as staying current. Those two things are drifting further apart as new substances enter the market faster than regulatory bodies can respond.
My advice: review your panel configuration annually. Not because regulations changed, but because the drugs your patients are using probably did.
— Justin
Drug test panels built for healthcare organizations

Healthcare organizations need panels that match their actual clinical environment, not a generic pre-employment screen designed for corporate HR programs. Rapidtestcup carries a full range of professionally configured drug test panels built for clinical, forensic, and compliance-focused applications.
The 12-panel ADLTX cup is one of the most popular options for substance abuse programs and clinical settings, covering 12 drug classes with built-in adulterant detection in a CLIA-waived format. For organizations managing high-risk populations or forensic cases, the 22-panel drug test with adulterants and Zaza covers a breadth of substances that no standard panel matches, including tianeptine, which is rapidly emerging as a clinical concern. The 15-panel option with adulterants hits the sweet spot for pain management clinics needing fentanyl, ketamine, and buprenorphine targets without moving to a full forensic configuration. All products ship quickly and qualify for bulk pricing.
FAQ
What is a screening panel in simple terms?
A screening panel is a grouped set of tests run on a single specimen to detect multiple substances or conditions at once. In drug testing, it means one urine sample can be checked for 5, 12, or even 22 different drug classes simultaneously.
How is a screening panel different from a single drug test?
A single drug test targets one substance. A screening panel targets multiple substances in one workflow, which improves efficiency, reduces specimen handling, and gives a more complete picture of a patient’s substance use or health status.
What does a positive screening panel result mean?
A presumptive positive means the targeted substance was detected above the cutoff threshold. It is not a confirmed result. All positive screens from an immunoassay-based panel require confirmatory testing by GC-MS or LC-MS/MS before any clinical or employment action is taken.
Why do different states have different screening panels for newborns?
The U.S. Recommended Uniform Screening Panel sets federal guidance, but states are not required to implement all conditions. Only 2 of 56 state and territorial programs screen for all 38 core conditions, meaning a newborn’s panel depends significantly on where they are born.
Are patients required to submit to screening panel testing?
No. Screening tests are voluntary, and patients retain the right to refuse. Informed consent is a legal and ethical requirement before any screening occurs, including in high-volume clinical or occupational health settings.