Blog
Why laboratory confirmation matters for drug test accuracy

TL;DR:
- Screening tests are rapid, affordable tools for high-volume drug testing, but they are not definitive. Confirmatory laboratory tests like GC/MS and LC/MS are essential when results influence high-stakes clinical, legal, or disciplinary decisions to ensure accuracy. Implementing clear workflows and medication reconciliation processes reduces errors, enhances legal defensibility, and improves patient care outcomes.
Screening tests are fast, affordable, and practical for high-volume settings. That’s exactly why so many treatment centers lean on them heavily. But speed and practicality don’t equal reliability when the stakes are high. A positive immunoassay result is presumptive, not definitive, and building patient care decisions, discharge plans, or legal documentation on presumptive data creates real risk. Understanding when and why laboratory confirmation must follow screening is one of the most important competencies a substance abuse treatment center can develop.
Table of Contents
- Why screening alone isn’t enough: Common pitfalls and risks
- Understanding laboratory confirmation: What it does and when it matters
- When to trigger confirmatory testing: Practical workflow for treatment centers
- Integrating medication reconciliation and lab interpretation: Avoiding edge-case errors
- The overlooked impact of confirmation: What most protocols miss
- Connecting the dots: Reliable test tools for your center
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Screening is not sufficient | Immunoassay screens alone can mislead and require careful interpretation. |
| Laboratory confirmation reduces risk | Confirmation testing acts as a safety net for high-stakes situations and disputed results. |
| Workflow triggers matter | Clear policies on when to confirm results improve quality and legal defensibility. |
| Medication reconciliation is essential | Reviewing medications and lab interpretation together minimizes cross-reactivity errors. |
Why screening alone isn’t enough: Common pitfalls and risks
Immunoassay screening tests work by detecting antibody reactions to drug compounds or their metabolites in urine. They’re designed to be sensitive, which means they cast a wide net. That sensitivity is useful, but it also means the net catches things you didn’t expect.
The most clinically significant problem is cross-reactivity. Many common medications share enough structural similarity with illicit drugs that the assay can’t tell them apart. A patient taking quetiapine may screen positive for methadone. Someone on bupropion may show a false positive for amphetamines. Dextromethorphan, found in over-the-counter cough syrup, is a well-documented cause of false positives on PCP screens. These aren’t rare edge cases. In a treatment population where patients often have complex medication regimens, cross-reactivity is a daily operational concern.
False negatives are just as dangerous. Some drugs are present in urine primarily as metabolites, and certain assay formats target only the parent compound. If the screen isn’t calibrated for the right analyte, it may miss a drug entirely even when that drug was consumed. Accurate interpretation requires understanding the assay’s target (parent vs metabolite) and that positive presumptive results should be interpreted with the patient’s current medications, because false negatives can be common depending on the drug or metabolite tested.
The most common pitfalls clinicians and administrators encounter include:
- Accepting presumptive positives without checking the patient’s medication list
- Using panel types that don’t detect current synthetic drugs or newer substance classes
- Failing to document the difference between a screening result and a confirmed result in patient records
- Treating a single negative screen as proof of abstinence without clinical context
“A positive immunoassay screen is a signal, not a verdict. Treating it as a verdict without confirmation is where preventable clinical and legal errors begin.”
The consequences of acting on an unconfirmed screen can be serious: wrongful discharge from a treatment program, incorrect medication adjustments, or flawed reports submitted to courts or probation officers. Strategies for managing false positives are essential reading for any clinical team that makes decisions based on urine drug screening results.
Understanding laboratory confirmation: What it does and when it matters
Laboratory confirmation is a second-tier test performed when a presumptive screening result needs to be verified or ruled out. It uses targeted analytical chemistry rather than antibody reactions, which means it can identify specific drug compounds with far greater precision.
The two most common methods are Gas Chromatography/Mass Spectrometry (GC/MS) and Liquid Chromatography/Mass Spectrometry (LC/MS). Both work by separating the components of a urine sample and measuring their molecular weight and structure. GC/MS has been the gold standard for decades. LC/MS is increasingly favored because it handles a broader range of compounds and works well with thermally unstable substances. The key distinction from immunoassay screens is that these methods confirm identity, not just presence.
When does confirmation become mandatory rather than optional?
The StatPearls clinical resource is clear: treat confirmation as a risk-control step needed when results carry clinical meaning beyond a screening signal, such as contested outcomes, legal or disciplinary actions, or decisions with serious consequences.
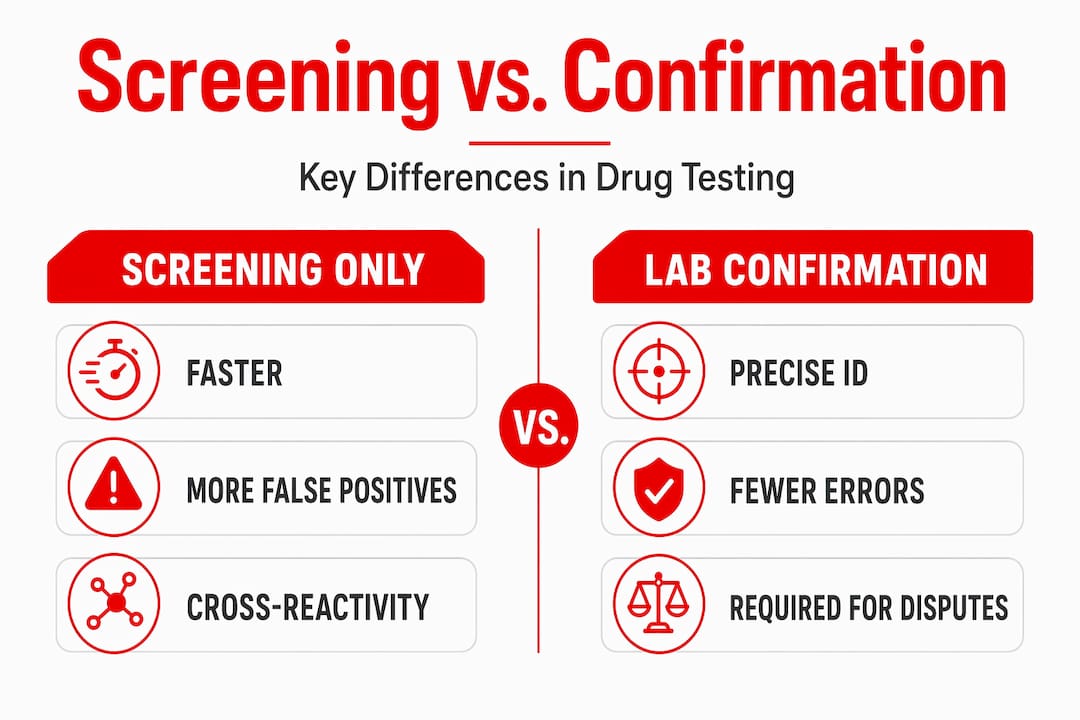
Here’s a practical comparison of screening vs confirmation:
| Feature | Immunoassay screening | Laboratory confirmation (GC/MS or LC/MS) |
|---|---|---|
| Speed | Minutes to hours | 24 to 72 hours |
| Cost | Low | Higher |
| Specificity | Moderate (cross-reactivity risk) | Very high |
| Legal defensibility | Low | High |
| Identifies specific compounds | No | Yes |
| Best use | Initial triage | Verification of presumptive results |
Common situations that require laboratory confirmation:
- A patient disputes a positive result
- The positive screen conflicts with the patient’s known medication list
- The result will be submitted to a court, parole board, or child protective services
- A treatment decision (discharge, medication change, step-down) hinges on the test outcome
- The patient is in a medication-assisted treatment (MAT) program where the presence or absence of specific opioids is clinically critical
Pro Tip: When a patient disputes a positive screen, document it immediately and send the specimen for GC/MS or LC/MS confirmation before taking any administrative action. Acting on an unconfirmed disputed result exposes your facility to significant liability.
For treatment centers evaluating their current approach, a detailed comparison of instant vs lab drug tests can help map screening tools to clinical contexts and identify where your workflow may have gaps.
When to trigger confirmatory testing: Practical workflow for treatment centers
Most treatment centers don’t have a clear written policy that specifies when a screen must be confirmed. That gap is where errors happen. The goal is to build a workflow that removes ambiguity from front-line staff and creates consistent, defensible documentation practices.
A well-designed workflow identifies specific trigger points rather than leaving the decision to individual judgment. The StatPearls guidance is direct: immunoassay screening may be sufficient for low-stakes clinical workflows, but confirmation becomes critical when presumptive results are disputed or when the decision environment is legally or administratively sensitive, such as workplace, court, or similar settings.
| Trigger type | Example scenario | Confirmation required? |
|---|---|---|
| Disputed positive | Patient claims result is wrong | Yes, always |
| Legal or court involvement | Probation compliance testing | Yes, always |
| Medication conflict | Positive amphetamine in patient on ADHD medication | Yes |
| MAT program monitoring | Buprenorphine presence or absence | Yes |
| Discharge decision | Positive screen used to justify discharge | Yes |
| Routine monitoring, no dispute | Weekly screen with no clinical action | Situational |
Key workflow practices to formalize in your center’s policy:
- Separate the roles. The person collecting the specimen should not be the person interpreting the result. This reduces bias and documentation errors.
- Use chain-of-custody forms for all specimens sent to confirmation. This is non-negotiable for legal defensibility.
- Set turnaround time expectations. Let clinical staff and patients know that confirmatory testing takes longer and that no administrative action will be taken until results return.
- Retain split specimens when possible. Some collection protocols allow the specimen to be split so one portion goes to initial confirmation and a second can be re-tested if contested.
Building a reliable workflow for compliance doesn’t mean slowing down your entire operation. It means defining clearly which situations require the extra step and making that extra step a standard procedure rather than an exception.
The appeal of rapid screening methods for high-volume settings is real. Point-of-care screens are fast and cost-effective, and they work well as the first layer. The issue arises when the first layer becomes the only layer. A multi-tiered system that uses rapid screens to triage and laboratory confirmation to verify doesn’t have to be slow, it has to be systematic.
Integrating medication reconciliation and lab interpretation: Avoiding edge-case errors
Even when a center has strong confirmation policies in place, errors still occur if the clinical team lacks the tools to interpret results in context. Medication reconciliation, the process of reviewing a patient’s complete current medication list before interpreting a drug test, is the missing link in many facilities.
Here’s why this matters operationally. A patient in your MAT program is on buprenorphine, clonazepam (prescribed), and gabapentin. Their urine screen returns positive for benzodiazepines. Is that a violation? Not necessarily. Without medication reconciliation, a staff member may flag the result as a program violation. With reconciliation, the team recognizes the clonazepam is prescribed, documents accordingly, and moves on. The StatPearls clinical framework supports this directly: build processes that integrate medication reconciliation and lab-result interpretation with confirmatory testing triggers, because cross-reactivity and targeted analyte design (parent vs metabolite) can both lead to presumptive errors.
A reliable medication reconciliation and interpretation process includes:
- Collect a complete medication list at intake and update it at each visit. Include prescriptions, over-the-counter medications, and supplements.
- Flag medications known to cause cross-reactivity before running a screen. Your lab or testing vendor should be able to provide cross-reactivity reference data for their assay panels.
- Train clinical interpreters, not just collectors. The staff member who reads the result needs to understand what the assay targets and what commonly causes interference.
- Create a formal escalation path. If a result conflicts with the medication list, there should be a documented process for who reviews it and what confirmation step follows.
- Document interpretation notes in the patient record. A positive result that was resolved through medication reconciliation should be documented as such, with the rationale.
Pro Tip: Assay cross-reactivity data is not always on the package insert. Contact the manufacturer directly or work with a lab that uses LC/MS confirmation so the reference data matches your actual screening chemistry. This alignment significantly reduces edge-case interpretation errors.
Understanding immunoassay screening principles at a deeper level helps your team recognize not just what a screen tests for, but how the antibody mechanism creates vulnerability to interference. And when those vulnerabilities appear, drug testing accuracy protocols backed by solid confirmation workflows are what protect both patients and the facility.
The overlooked impact of confirmation: What most protocols miss
Most clinical protocols treat laboratory confirmation as a fallback. Something you use when a result is challenged or when a lawyer gets involved. That framing undersells what confirmation actually does for patient care and organizational risk.
Here’s the uncomfortable reality: many treatment centers have discharged patients, altered MAT dosing, or submitted compliance reports based solely on immunoassay screens that were never confirmed. Some of those results were wrong. The harm caused by acting on a false positive or missing a false negative doesn’t always surface immediately. It might appear months later in a licensing review, a malpractice claim, or a patient readmission that could have been prevented.
What confirmation does strategically is reduce the decision error rate for your highest-stakes cases. It’s not about doubting your screening tools. A good rapid screen is still the right starting point. It’s about recognizing that the cost of a confirmatory GC/MS or LC/MS test is almost always lower than the cost of acting on bad data, especially when that data triggers a consequential decision.
The confirmatory drug testing literature reinforces this repeatedly: confirmation should be routine for any result that informs a clinical or administrative action with lasting consequences, not a last resort when someone complains. Reframing it that way changes how your staff thinks about the step. It stops being bureaucratic and starts being protective.
Treatment centers that build confirmation into their standard operating procedures, rather than treating it as exceptional, tend to have fewer contested outcomes, cleaner legal documentation, and more defensible records during audits. The protocol change isn’t expensive. The cost is in not having it.
Connecting the dots: Reliable test tools for your center
Quality testing starts with the right equipment at the screening stage and depends on disciplined protocols at every step that follows.

At Rapid Test Cup, we stock the tools that support a complete, multi-tiered drug testing workflow. The 12 panel test cup gives you a solid, CLIA waived first-line screen across the most commonly abused substance categories. For broader panel coverage in high-complexity cases, the 22 panel test cup includes adulterant detection and extended drug classes including Zaza, giving your clinical team more information to act on. For targeted confirmatory workflows, the MET drug test strip supports focused methamphetamine screening with the specificity your confirmation protocols require. Quality screening products, combined with clear confirmation triggers, are the foundation of accurate, defensible drug testing in any treatment setting.
Frequently asked questions
How do laboratory confirmation methods work in drug testing?
Laboratory confirmation uses advanced analytical techniques like GC/MS or LC/MS to reliably identify drugs by molecular structure, eliminating the cross-reactivity errors that affect immunoassay screens.
When should confirmatory testing be triggered in treatment centers?
Confirmatory testing is required whenever presumptive results are disputed or when results feed into legally or administratively sensitive decisions like court compliance reports, discharge, or MAT dosing adjustments.
What are the main causes of false positives or negatives in drug screening?
False positives and negatives are primarily caused by assay cross-reactivity and mismatches between the assay’s target analyte and the actual drug compound or metabolite present in the specimen.
How does medication reconciliation impact drug test interpretation?
Medication reconciliation identifies prescriptions that may cause cross-reactivity, and integrating it with confirmation triggers prevents misinterpretation of results that would otherwise appear to indicate illicit drug use.